Excipients/Inactive Ingredients: nicorette icy mint 2mg gum · nicotine (as resinate): Chewing gum base, levomenthol, acesulfame potassium, talc, magnesium oxide (light), xylitol, peppermint oil, sodium carbonate anhydrous, and sodium hydrogen carbonate.
nicorette icy mint 4mg gum · nicotine (as resinate): Chewing gum base, xylitol, levomenthol, quinolone yellow E104 Al-lake, acesulfame potassium, magnesium oxide (light), peppermint oil, sodium carbonate anhydrous, and talc.
Pharmacotherapeutic group: Drug used in nicotine dependence. ATC code: N07B A01.
Pharmacology: Pharmacodynamics: Abruptly interrupted use of tobacco products after a long period of daily use may give characteristic withdrawal symptoms comprising four or more of the following: dysphoria or depressed mood, insomnia, irritability, frustration or aggression, anxiety, difficulty in concentrating, restlessness or impatience, reduced heart rate, increased appetite or increase in weight. Urge to smoke is recognized as a clinically relevant symptom, and is an important part of the withdrawal symptoms when giving up smoking.
Clinical studies have shown that nicotine replacement products can help smokers abstain from or reduce their smoking by relieving these withdrawals symptoms.
Pharmacokinetics: The amount of nicotine absorbed from a piece of nicotine chewing gum depends on the quantity of nicotine that is released into the oral cavity and the amount that is lost via swallowing. The greater part of nicotine that is released is absorbed through the oral mucosa. The systemic bioavailability of swallowed nicotine is lower because of first-passage elimination. The high and rapidly rising nicotine concentrations that are seen with smoking are seldom reached with treatment with chewing gum.
In normal case, approximately 1.4mg of nicotine is released from a 2mg piece of chewing gum and approximately 3.4mg nicotine from a 4mg piece of chewing gum. Maximum blood concentration is achieved after 30 minutes of chewing and is then comparable to the concentration 20-30 minutes after smoking a cigarette of medium strength. The volume of distribution after intravenous administration of nicotine is around 2 to 3 L/kg and the half-life is approximately 2-3 hours.
The major eliminating organ is the liver, although the lungs and brain also metabolise nicotine to a small extent. The enzyme primarily involved in biotransformation of nicotine is CYP2 A6. Seventeen metabolites of nicotine have been identified, all of which are believed to be less active than the parent compound. The primary metabolite of nicotine in plasma, cotinine, has a half-life of 14-20 hours and concentrations that exceed nicotine by 10-fold. The plasma protein binding of nicotine is considered to be low, about 5%.
Other diseases or concomitant use of other drugs which affect the level of plasma proteins are not expected to have a significant effect on the nicotine kinetics. The main metabolites in urine are cotinine (10-12% of the dose) and trans-3-hydroxy cotinine (28-37% of the dose). Approximately 10-15% of the nicotine is excreted unchanged with the urine. Up to 23% may be excreted with the urine via increased diuresis and acidification of the urine below pH 5.
Greatly impaired renal function is assumed to affect total clearance of nicotine. Elevated nicotine levels have been seen in smoking subjects undergoing haemodialysis.
The pharmacokinetics of nicotine are unaffected in liver cirrhosis patients with mild impairment of liver function (Child-Pugh score 5) and reduced by about 40-50% in liver cirrhosis patients with moderate impairment of liver function (Child-Pugh score 7).
A smaller reduction in total clearance of nicotine has been shown in healthy elderly users, however, not justifying adjustment of the dose.
No difference in nicotine kinetics has been observed between men and women.
Nicorette is used for the treatment of tobacco dependence by relieving nicotine craving and withdrawal symptoms. Facilitating smoking cessation in smokers motivated to quit.
As an aid to reduce smoking [Nicotine Assisted Reduction to Stop (NARS)].
Stop smoking completely at the same time in order to increase your chances of success. Regular use beyond 12 months is generally not recommended.
Adults: The initial dosage should be individualized on the basis of the smoker's nicotine dependence. The Nicorette chewing gum 4mg is recommended for smokers who are highly dependent (for example smoking 20 cigarettes or more per day or smoking the first cigarette in the morning 30 minutes or less after waking up). Other smokers should begin treatment with the 2mg dosage strength.
The Nicorette chewing gum should be used when cigarettes normally would have been smoked or if cravings emerge. Sufficient Nicorette chewing gum should be used each day. In order to maximize the chances of success it is important not to underdose. The dosage should be individualized on the basis of the smoker's nicotine dependence.
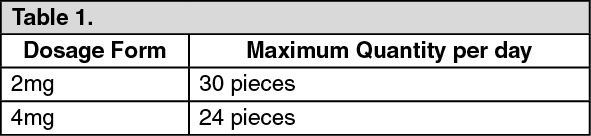
Dosing regimen: 8 to 12 Nicorette chewing gum per day, for at least 3 months. Do not exceed the following number of gums as stated as follows in any 24-hour period. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Smokers should stop smoking completely during the course of treatment with Nicorette chewing gum.
Gradual tapering from the Nicorette chewing gum should then be initiated. Treatment should be stopped when the dose is reduced to 1 to 2 Nicorette chewing gum per day.
Each piece of Nicorette chewing gum should be chewed slowly for approximately 30mins, with pauses. The gum should be chewed until a strong taste or mild burning sensation is experienced, then rested between the cheek and gums until the taste and/ or sensation have disappeared, then chew again slowly and repeat.
Children and adolescents: Do not administer Nicorette chewing gum to persons under 18 years of age without recommendation from a health care professional.
Combination therapy: Highly dependent smokers, smokers who experience "breakthrough" cravings or those who have failed with single NRT treatment, can use a flexible smoking cessation format, in combination with the patch for fast relief of cravings.
Administration of nicotine should be stopped temporarily if any symptoms of nicotine excess occur. Nicotine intake should be decreased by either lowering dosing frequency or strength if nicotine excess symptoms persist.
Route of administration: Oral.
Symptoms of overdosage with nicotine may occur if patient has low nicotine consumption before the treatment or uses other sources of nicotine at the same time.
The symptoms of overdose are those of acute nicotine poisoning and include nausea, vomiting, increased salivation, abdominal pain, diarrhea, sweating, headache, dizziness, disturbed hearing and marked weakness. At high doses, these symptoms may be followed by hypotension, weak and irregular pulse, breathing difficulties, prostration, circulatory collapse and general convulsions.
Doses of nicotine that are tolerated by adult smokers during treatment may produce severe symptoms of poisoning in small children and may prove fatal. Suspected nicotine poisoning in a child should be considered a medical emergency and treated immediately.
Administration of nicotine must be stopped immediately and the patient should be treated symptomatically. If excessive amount of nicotine is swallowed, activated charcoal reduces the gastrointestinal absorption of nicotine.
Hypersensitivity to nicotine or any excipients in the chewing gum.
Smokers who wear dentures may experience difficulty in chewing Nicorette chewing gum. The chewing gum may stick to, and may in rare cases damage dentures.
A risk-benefit assessment should be made by an appropriate healthcare professional for patients with the following conditions: Dependent smokers with a recent myocardial infarction, unstable or worsening angina including Prinzmetal's angina, severe cardiac arrhythmias, recent cerebrovascular accident, and/or who suffer with uncontrolled hypertension should be encouraged to stop smoking with non-pharmacological interventions (such as counselling). If this fails, the Nicorette chewing gum may be considered but as data on safety in this patient group are limited, initiation should only be under close medical supervision.
Patients with diabetes mellitus should be advised to monitor their blood sugar levels more closely than usual when smoking is stopped and NRT is initiated, as reductions in nicotine-induced catecholamine release can affect carbohydrate metabolism.
Use with caution in patients with moderate to severe hepatic impairment and/or severe renal impairment as the clearance of nicotine or its metabolites may be decreased with the potential for increased adverse effects.
Use with caution in patients with uncontrolled hyperthyroidism or phaeochromocytoma as nicotine causes release of catecholamines.
Nicotine may exacerbate symptoms in patients suffering from oesophagitis, gastric or peptic ulcers and NRT preparations should be used with caution in these conditions.
Doses of nicotine tolerated by smokers can produce severe toxicity in children that may be fatal. Products containing nicotine should not be left where they may be handled or ingested by children, see Overdosage.
Nicotine dependence may continue but at a lower level. However use of pure nicotine is less harmful than tobacco.
Pregnancy: Nicotine passes to the foetus and affects its breathing movements and circulation. The effect on the circulation is dose dependent. Therefore, the pregnant smoker should always be advised to stop smoking completely without use of nicotine replacement therapy. The risk of continued smoking may pose greater hazard to the foetus as compared with the use of nicotine replacement products in a supervised smoking cessation programme. Use of Nicorette Chewing Gum by the pregnant smoker should only be initiated after advice from a health care professional.
Lactation: Women should take the product just after having breastfeeding. Nicotine passes freely into breast milk in quantities that may affect the child even with therapeutic doses. Nicorette chewing gum should therefore be avoided during breast-feeding. Should smoking cessation not be achieved, use of the Nicorette chewing gum by breast feeding smokers should only be initiated after advice from a health care professional.
Most of the undesirable effects reported by the subjects occur during the early phase of treatment and are mainly dose dependent. Irritation in the mouth and throat may be experienced, however most subjects adapt to this with ongoing use. Allergic reactions (including symptoms of anaphylaxis) occur rarely during use of Nicorette chewing gum.
As would be expected, the types of adverse reactions seen for the chewing gum in clinical trials are similar to those associated with nicotine administered by other means.
Clinical Trial Data: The safety of nicotine from clinical trial data is based on data on a meta-analysis of randomized clinical trials (RCTs) for the treatment of smoking cessation.
ADRs with oral formulations identified from clinical trials are presented as follows in Table 2. (See Table 2.)
Click on icon to see table/diagram/image
Post Marketing Data: Adverse drug reactions first identified during post-marketing experience with nicotine are presented in Table 3. Frequencies are provided according to the following convention: Very common ≥1/10; Common ≥1/100 and < 1/10; Uncommon ≥1/1,000 and < 1/100; Rare ≥1/10,000 and <1/1,000; Very rare <1/10,000; Not known (cannot be estimated from the available data). (See Table 3.)
Click on icon to see table/diagram/image
Undesirable effects that may arise from combination treatment (chewing gum and patch) differ from each treatment alone only with regards to local undesirable effects that may be attributed to pharmaceutical form. The frequency of these undesirable effects is comparable with that given in the summary of product characteristics for the respective product.
Smoking (but not nicotine) is associated with increased activity of CYP1A2. After giving up smoking, clearance of certain medications which are metabolized via CYP1A2 may be reduced. This may lead to increased plasma levels of certain medications. The increase may be of clinical significance for products with narrow therapeutic windows, e.g. theophylline, tacrine, clozapine or ropinirole.
Plasma level of other medications which are in part metabolized via CYP1A2, e.g. imipramine, olanzapine, clomipramine and fluvoxamine, might also rise after stopping smoking. There are no data supporting this, however, and the possible clinical significance of this effect on these medications is unknown.
Limited data indicates that the metabolism of flecainide and pentazocine might also be capable of being induced by smoking.
No clinically relevant interactions between nicotine replacement therapy and other drugs has definitely been established. However, nicotine may possibly enhance the haemodynamic effects of adenosine i.e. increase in blood pressure and heart rate and also increased pain response (angina-pectoris type chest pain) provoked by adenosine administration.
Dispose of the chewing gum sensibly.
Do not store above 30°C.
Protect from light.
N07BA01 - nicotine ; Belongs to the class of drugs used in the management of nicotine dependence.
Nicorette Icy Mint Gum chewing gum 2 mg
105's
Nicorette Icy Mint Gum chewing gum 4 mg
105's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image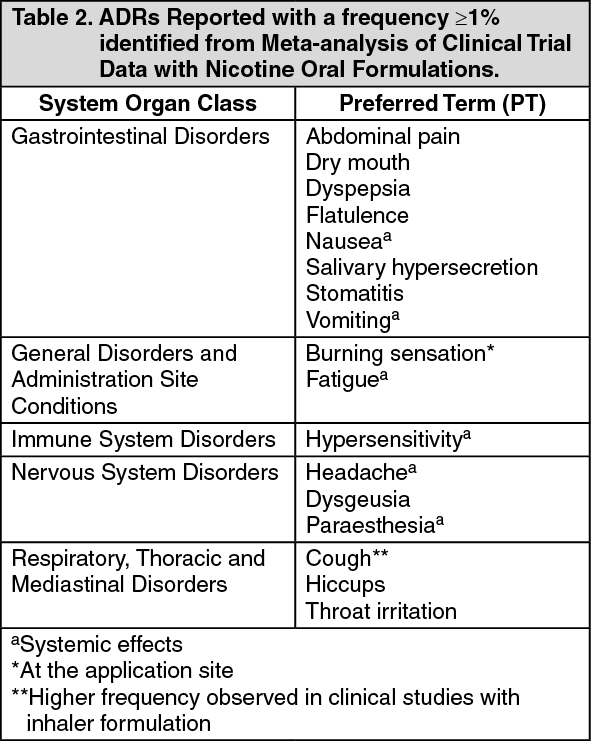 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image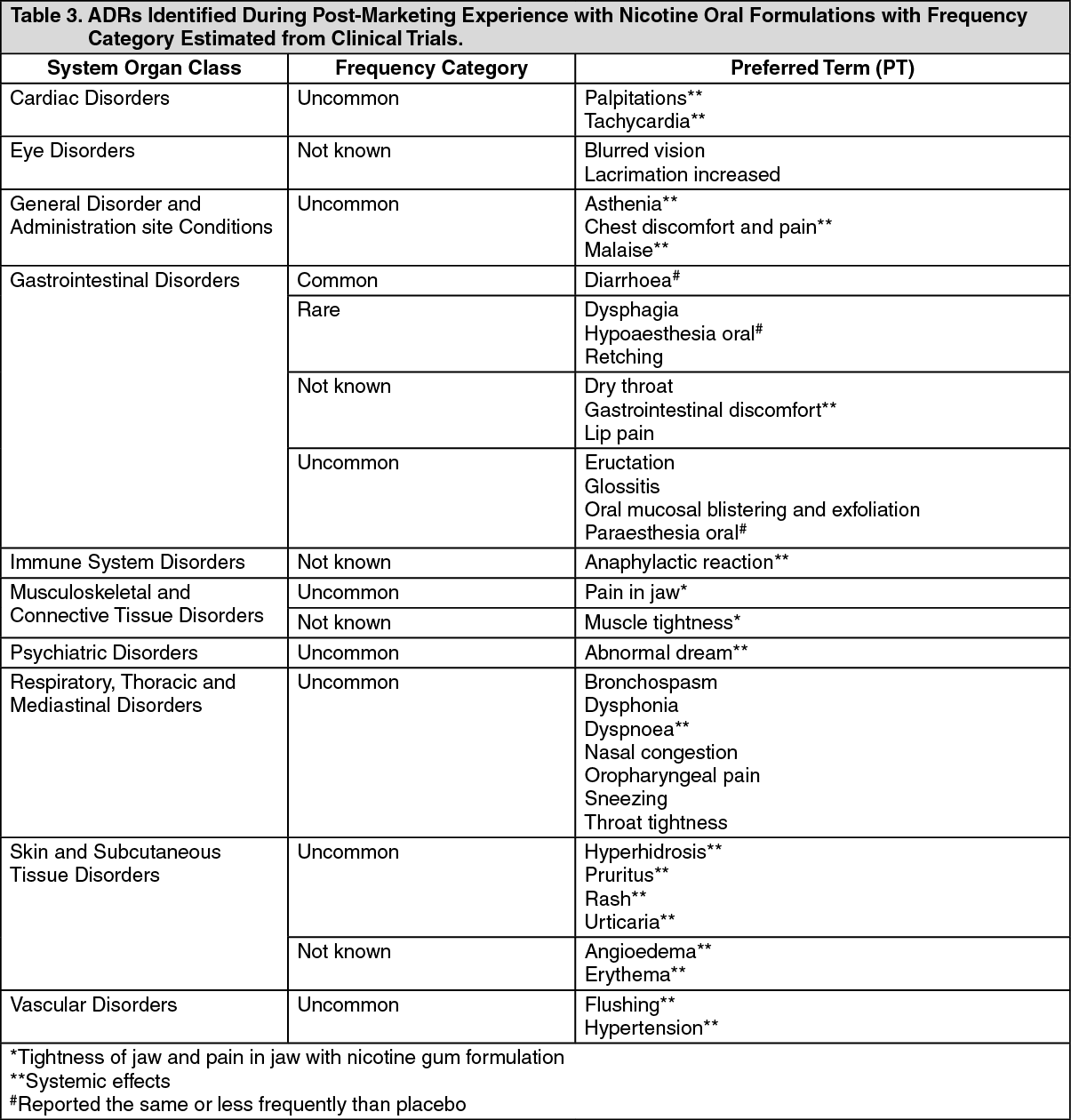 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
